About one in 7 couples (15%) are affected by infertility.

Healthy couples in their 20's have a one in four chance of getting pregnant each month.
About 40% to 50% couples get pregnant within 4-5 months and 85% get pregnant within 12 months.
When a couple has been trying to get pregnant unproductively for at least 1 year, and if the woman is 35 years or older, the analysis is mainly infertility.
It is usually a responsibility of both partners, one-third of infertility cases are related to the man's problems, one-third to the woman's and in one-third of cases both are responsible. In about fifteen percent of infertility cases no cause is found (unexplained infertility).
Healthy sperm by the man
Enough sperm by the man
Healthy eggs produced by the woman
Healthy and unblocked fallopian tubes that allow the sperm to reach the egg
The sperm's ability to fertilize the egg when they join
The ability of the fertilized egg (embryo) to become implanted in the woman's uterus
The ability of the lining of the uterus to allow implantation
Sufficient embryo quality
A healthy embryo
A healthy hormonal environment of the woman

(sperm problems: Not enough, not moving, bad shapes)
Factors (PCOS or age related issues, Good eggs versus not-so good eggs)
(infections, endometriosis, scar tissue)

(Kallmann syndrome, fragile X syndrome, karyotype abnormalities, ciliary dyskinesia)
(Antisperm antibodies, antiovary antibodies, prevention of embryo cleavage)
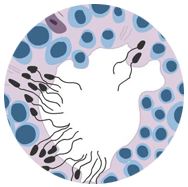
Oligospermia is one of the main causes of male infertility or sub-fertility The word Oligispermia means when a man has low sperm count in his semen, this is tested by a test called Semen Analysis. Treatment varies depending on the type and severity of oligospermia, the individual case, and the presence of complications. Treatment may include improving the diet, losing or gaining weight as needed, not smoking, reducing alcohol intake, and avoiding hot tubs, tight underwear, and other factors that may create excessive heat around the testicles and reduce sperm count. In oligozoospermia there are fewer sperm cells in the ejaculate than normal. If a male person suffers from olispermia it is difficult for the women to conceive naturally in spite of her being fertile .Once detected , the couple should visit an infertility specialist rather than wasting time , the treatement ahead cured through medication or ART procedures. Often semen with a decreased sperm concentration may also show significant abnormalities in sperm morphology and motility.
Azoospermia means no sperm in the semen sample, it is associated with infertility, it is diagnosed on the absence of the sperm after the centrifugation of complete semen specimens using microscopic analysis. History and physical examination and hormonal analysis (FSH, testosterone) are undertaken to define the cause of azoospermia.It is a frequent contributing factor towards inability to naturally conceive. Azoospermia doesn’t necessarily mean that , the patient cant conceive there are treatment available , its just you have to go to the right place at the right time of life .There are surgical procedures like TESE/PESA, where sperm are exacted from the testes of man reproductive organ . One good sperm found would help help in getting pregnant through ART methods like IVF, ICSI.summary, a thorough evaluation of the male is an integral part of the overall fertility evaluation. Diagnostic testing is easy, and there are many effective treatments available – even in the most severe cases.
Normal sperm are quick and as soon as they are ejaculated, they swim as fast as possible through the vagina into the fallopian tube in order to fuse with the egg and to fertilize it. The term motility means movement of the sperm. if the movement of the sperm is sluggish or not in a straight line or not swimming properly, it will be hard to invade the cervical mucus, or penetrate the egg preventing pregnancy .There are many causes of Low motility , some of them are –stress, heat, eating and drinking hobbits , medication , genetics , Overabundance of sex,etc. While sperm count plays an important role in determining a man’s fertility, the motility of the sperm carries just as much weight.Low sperm motility does not mean end of the journey towards conception .If, after making appropriate changes to your lifestyle, you continue to struggle with low sperm motility, there are treatments available such as IUI, IVF, ICSI.
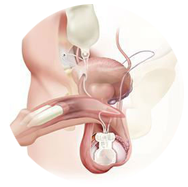
The vas deferens connects the sperm-producing testicles to the penis. Therefore, those who are missing both vas deferens are typically able to create sperm but are unable to transport them appropriately. As a result, men with this condition are unable to father children (infertile) unless they use assisted reproductive technology .It can be diagnosed through Scrotal ultrasonography and transrectal ultrasonography., Individuals with CAVD can reproduce with the assistance of modern technology with a combination of testicular sperm extraction and intracytoplasmic sperm injection(ICSI). However, as the risk of either cystic fibrosis or renal agenesis is likely to be higher in the children, genetic counselling is generally recommended. Fortunately, nowadays patients who have CAVD can have optimistic expectations of successful reproduction.
The testicals make male hormone including testosterone and produce sperm, the male reproductive cells. Testicular failure is when the sperm cannot be produced thereby preventing fertilization or pregnancy. The causes are certain drugs, mumps, orchitis and testicular cancer or injury to the testicals.Problem with the testis leads to hormonal imbalance, sexual problems and infertility. Symptoms can be decrease in height, enlarged breast, infertility, lack of sex drive. Testicular dysfunction and low testerone levels are hard to diagnosis in older men as the testerone levels falls with age..Many forms of testicular failure cannot be detectected.Hormone replacement therapy can help reverse symptoms, although it may not restore fertility.
Hormones are chemical messengers that travel through the bloodstream to the organs and tissues. They tell our organs what to do and how to function. Hormones are made by endocrine glands, which are special groups of cells found throughout the body. The main endocrine glands are: Male hormonal problem is a growing problem in men. Although testosterone is considered a male hormone, estrogens also affect men. The problem occurs when the testosterone level is reduced whereas the estrogens are increased. When men get older, they experience a decline in testosterone. This is better known as andropause, or male menopause. Both estrogens and testosterone need to be kept in balance for women and men. The causes are for the imbalance can be due to chronic kidney or liver deasese, autoimmune diseases, mumps, heart failure, HIV, stess, alcohol, and other lifestyle related issues. Symptoms are Fatigue, lack of energy, mood swings, hairloss, and muscle weakness. Doctors can prescribe certain tests to determine exactly which type of hormone imbalance you’re suffering from.
An ovulation disorder is any condition that effects the normal ovulation process which is necessary to conceive other factors such as stress and diet can adversely affect ovulation so you should not assume ovulation disorder just because your attempt to conceive have been unsuccessful, in normally fertile couple there is a 25 percent chance of getting pregnant each cycle, meaning that about 75 to 85 percent women who have regular unproductive sex will get pregnant within a year. A fertility specialist will determine whether you have an ovulation disorder that is affecting your ability to conceive. A women with an ovulation (absent ovulation)A condition in which the follicles or her ovaries does not release eggs or she may have oligoovulation,in which ovulation is irregular/in frequent but not completely absent. A menstrual cycle that is shorter than 21 days and longer than 21 days is assign of ovulation dysfunction. Another sign of ovulation dysfunction is the length of a women cycle fluctuates from month to month. Infertility and hormonal irregularities is another sign that an ovulatory dysfunction may be present. Fortunately, many disorders can be treated; the type of treatment that will be administered will depend on the cause. Medical and non surgical treatment may include nutritional adjustment, ovulation-inducing fertility medicines and stress reduction.
An imbalance in hormone is usually caused by high stress, insufficient sleep, unhealthy diet, diabatese menopause, pregnancy, thyroid problems and other conditions. The body has a very delicate chemistry and changes can produce noticeable symptoms and other health problems. While a hormonal imbalance is frustrating and difficult experience there is help.
Various treatment, medications and lifestyle treatment may be successful in addressing hormonal imbalance. Hormonal fluctuations occur naturally such as in puberty, menopause or premenopausal conditions. Hormones are essential to overall wellbeing they relay chemical messages throughout the body, helping to keep your emotions and body in check, one of the key body systems affected by the balance of hormones in your body is the reproductive system. It causes heavy period s, infertility, and endometriosis. The most common medical treatment of hormonal imbalance is the prescription of bio identical or synthetic hormone, this is known as hormone replacement therapy. Conventional treatment for hormonal imbalance includes synthetic hormone replacement therapy, birth control pills, insulin injections, thyroid medications and others.
The number and quality of eggs (ovarian reserve) may decrease at the age of 30 or earlier. They decrease rapidly after 40. But age is not the only reason that the number and quality of eggs decrease. Abnormalities in the ovaries can also cause such a decrease. In primary ovarian insufficiency (sometimes called premature menopause) the number of eggs in the ovaries decrease early , in a few women primarily ovarian insufficiency is the reason they have irregular menstrual periods or no periods. Reproduction is controlled by a system that includes the hypothalamus (a area of the brain ), pituitary gland , ovaries , and other glands such as the adrenal glands and thyroid glands .Other causes of ovulation problem include diabetes, obesity, excessive exercise, certain drugs (estrogens and progestins and anti-depressants, weight loss, physiological stress)
However reliable test for diagnosing egg production problems are Blood test like AMH (anti mullerian hormone) Ultrasound.
There are treatments available such as IVF or OD (OOCYTE OF A DONOR).
Marital fertility rates in natural populations (no contraception) as a function of age of wife. Ovaries from Indian women seem to age at an earlier stage (6 years) than Caucasian women.
In general, women's fertility begins to decline gradually after age 30, with a steep drop between 35 and 45. This means that, on average, it takes longer for an older woman to conceive, and older women are more likely to be diagnosed with infertility. Pregnancies in older women are also more likely to miscarry. The most predictable agerelated change is a gradual reduction in the number and quality of eggs produced as a woman enters her late thirties. As she nears menopause, eggs are not released in more and more of a woman’s menstrual cycles, making conception impossible . Also, as women age, they are more likely to have had illnesses or medical treatments that can compromise fertility. Some of these affect the reproductive system directly, such as endometriosis, sexually transmitted diseases (STDs), surgery on the reproductive organs, or ectopic pregnancies. Others are general medical problems that can damage fertility such as hyporthyrodism,high bloodpressure and lupus.as they age man may also be exposed to infections,medication enviromental chemicals that can impair fertility. However, they do not experience the same dramatic and predictable agerelated decline as women. Because of the increased possibility of fertility problems, women over the age of 35 are often counseled to seek medical advice if they attempt to conceive for six months without success. However, because conception is likely to take longer in older women, some experts suggest that couples give themselves more, rather than less, time to conceive before seeking medical help. Couples must find a balance between not allowing enough time for conception and delaying too long (making treatment less likely to succeed).
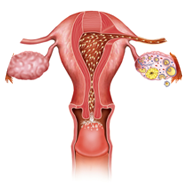
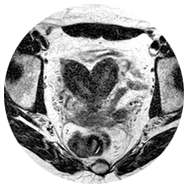
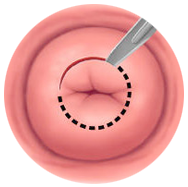
Fallopian tubes play an important role in female fertility. It gives the passage for spermatozoa to find the ovum, is the site for natural fertilization and helps the developing embryo find its way toward uterine cavity for implantation. The fallopian tubes need not just be patent anatomically but they should be functional physiologically also. Tubal infertility is a major reason of infertility. A normal tube should not be visible on ultrasound and when seen, it is always pathological. This would happen only if the tube is distended or edematous. A hydrosalpinx or a hematosalpinx will be seen as a tubular structure in theadnexa. It could be uniloculated, but mostly it appears like a multiloculated adnexal structure.
Each month when ovulation occurs, an egg is released from one of the ovaries, the egg travels from the ovary through the tubes into the uterus. The sperm needs to travel their way from the cervix through uterus and the fallopian tube to get to the egg . If one or both fallopian tubes are blocked the egg cannot reach the uterus and the sperm cannot reach the egg prevent fertilisation and preganancy. The most common cause of blockage of tube is PID.
Treatments – Laproscopic surgery.
Peritoneal and pelvic factor affecting fertility are either due to infection (pyogenic or tuberculosis) or endometriosis or due to past surgical procedures, which not only results in adhesion formation, which alters the peritoneal function affecting fertility by preventing oocyte release from the ovary. These adhesions can also inhibit ovum capture or transport by the fallopian tube. Embryo transport abnormalities increase the risk for ectopic pregnancy. There is increase in volume of peritoneal fluid with increased concentrations of prostaglandins, proteases and inflammatory cytokines leading to systemic inflammation. It can also result in endocrine and ovulatory abnormalities.
The peritoneal fluid environment hosts the processes of ovulation, gamete transport and survival, sperm-ovum interaction, early embryonic development as well as implantation. The various cellular and a cellular components of the peritoneal fluid, which is dynamic, are in a constant inter-active state, being influenced by the physiological events and pelvic disease processes.1 This again shows how important the peritoneal factor is to fertility.
If at the first pelvic examination and at ultrasound one suspects pelvic inflammatory disease (PID) or endometriosis or there is a history of previous abdominal or pelvic surgery, the peritoneal and pelvic factor should be assessed by laparoscopy earlier than when these comorbidities do not exist.
Are harmless tumours which grow in the uterus. The uterine wall is made of smooth muscle fibres. Fibroids are overgrowth of these fibres. Some 30% women have these in their lifetime. But only some of them suffer from infertility due to tumours. I read somewhere that 50% woman in Africa have such tumours. But is infertility that common there? At the same time, it is true that women with many tumours in uterus have infertility and repeated miscarriages. So, there is some relation between tumours and infertility even though it may not be linear that is as simple as cause and effect. Lot of paper and now internet space has been taken up with this issue. And still we are not clear as to the role that these tumours have in infertility. In very simplified terms which is of course not fully correct, tumours may cause hindrance to the implantation of embryos in the endometrial bed if they are present anywhere close to the bed. They create a so-called negative environment which hampers implantation. Reasons are poor endometrial blood supply near the fibroids or the tumours acting as foreign body hostile to embryo implantation.
It is easy to identify fibroids. A simple ultrasound may detect these tumours. We could also do a HSG/SSG to see the location of the tumour and whether they are impinging on to the endometrium. Based on that we do we may also recommend removal of these fibroids. Only the risks need to be evaluated against the possible benefits. Lot of western societies have set guidelines for their member doctors to follow. So it is very easy for both the patients and their treating doctors. But medicine cannot be cut paste application of formulae. So we need to go on a person to person basis. See the tumour location, number and size and then decide. I would try naturally for sometime with a woman who is 25, just married and no obvious cause of infertility but indeed ask for myomectomy who has failed two IVF before even with excellent embryos.
Adhesions are bands of scar tissue that can cause internal organs to be stuck together when they are not suppose to be , most often adhesions are the result previous surgery but some can occur following pelvic infections and many times they accompany more sever stage of endometriosis .Surgical procedures such as mymomectomy and endometriosis surgery can also lead to adhesions .Pelvic adhesions can cause a impact on a women ability to conceive and carry a baby to term. Pelvic adhesions are treated if they are causing bothersome symptoms by resection surgery, which removes the scar tissue. Removal of adhesions can be accomplished using laparoscopy or microsurgical techniques. Studies have shown removal of adhesion can reduce and can potentially improve the possibility of conceiving versus no treatment at all.
Antisperm antibodies
Antisperm antibody test looks for special proteins (antibodies that fight against a mans sperm in blood , vaginal fluids or semen .the test uses a sample of sperm and adds a substance that binds only 2 affected sperm . Semen can cause a immune system response in either the man and women’s body .Many couples on their path to parenthood encounter fertility issues such as endometriosis PCOS , uterine fibroids, blocked fallopian tubes, low sperm count , motility or any number of hormONal imbalance that may contribute to infertility, but one issue that is not talked about is antisperm antiobody .The immune system forms antibodies in response to antigens protecting sperm from contact with blood prevents the immune system from forming antibodies against the antigens (proteins )present on sperms . This antigens are alwaYS present and are harmless until they trigger antibody production In women there is some evidence that anti sperm antibodies are most often present but that we also have what are called (neutralising serum anti –idiotypic antibodies) which counteract the antisperm antibody, making them somewhat irrelevant .Some antibodies can cause sperm to clump together ,other antibodies can cause sperm to become targets for the women’s natural killer , some antibodies will cause sperm to become immobilised, soem will allow sperm to enter the cervix but then prevent the little swimmers form binding to the women’s egg and fertilising it, other may cause early miscarriage.
Tubal blockage is the least understood and most commonly made out reason for infertility. The fallopian tubes are mobile organs cylindrical in shape, attached to the uterus at one end and free at the other end. The free end has finger like projections which can catch the egg when it is released from the ovary. These eggs are then placed somewhere in the middle of the tube waiting for the sperms to reach. Now, if there are enough sperms which can make their way to the egg, then these sperms secrete two acids which dissolve the capsule around the egg allowing one sperm to go through into the egg to fertilize it. Thereafter, when the egg has become an embryo about 4-5 days old, there are hairs like projections (cilia) inside the lumen of the fallopian tube that push the embryo towards the other end into the uterine cavity for implantation. So, to reiterate, the tubes have three roles to play, pick up the egg, allow to sperms to come through and finally transfer the embryo to the uterine cavity. Two of these are dynamic activities which really cannot be assessed in any sure way. Only the fact that the sperms may not reach up to the egg can be commented upon by checking whether the tubes are open or not.
Tubes are open or not are again a little tricky to test. We do an hsg/ssg/ laparoscopy to find out tubal status. But as mentioned before none of them is accurate. In quite a few cases, we are no wiser after the procedure. In all of the above procedures we rely on pushing water/dye into the uterus hoping that if tubes are open some of it would trickle out through their free end. So while tubes are not open for innocent sperms as they have no pressure to put, they open up miraculously in HSG/SSG when we do apply pressure to push the water/dye in. This is a dichotomy to be remembered always.
Also while we keep emphasizing tubal patency, we forget that tubo-ovarian relationship is just as crucial. If the tube and the ovaries are far apart, or as I have been stating again and again, somehow the tube and the ovaries are sticking to the back of the uterus and none is mobile then it is more at fault for the egg not finding its way into the tube rather than tubal block.
The straight and simple answer for all tubal factor infertility is IVF. But we could attempt other things provided duration of marriage is less than 5 years and the female is young. Tubal cannulation is a technique where a fine malleable catheter (pipe) is introduced into the fallopian tube from inside the uterine cavity. As it passes, it may take care of occasional blocks in the tube and create a sort of inner passage within the fallopian tube which if it maintains can allow sperms eventually to get to the egg. But as mentioned earlier, the success rate in terms of a pregnancy is not very encouraging because if the tubes are really damaged then opening them does not solve the problem as the hair like structures are not ok and would not transfer the baby back to the uterus when needed. We should attempt this in young women who have no known reason for picking up tubal damage such as past abdominal infection, appendicitis, chronic pelvic infections, history of TB etc.
In all of rest, IVF currently offers the best possible chances at the least cost in terms of money and time.
Sometimes cases taken as unexplained infertility also eventually turn out to be tubal factor infertility. Because when we do IVF, we see that most of the eggs taken out have fertilized well and pregnancy happens quite easily with this technique whereas they had been toiling for last so many years with apparently everything ok.
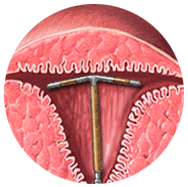
Is another reason for infertility, albeit a rare one. In women who have undergone previous surgeries such as dilation and curettage for any reason, there is risk of developing this sort of a block if the operation is not performed correctly or if there was some infection post surgery. At times hostile cervix is held out as the reason why you aren't conceiving. But I am not really convinced of this. The theoretical explanation is that the cervix remains plugged with thick gum like mucus for most of the days of the month. This plug is sort of a last barrier for the body’s defense. Because if any infective organism gets past this barrier it may damage the tubes and the like. Now this mucus plug has a lot of good and bad properties. As mentioned earlier, it holds back the infection. But there are conditions where the sperms which are supposed to be allowed in are also held back and that is not good for fertility. There are cells which secrete antibodies which are policemen like things which catch hold of the sperms and bind them not allowing them to enter the uterus (antisperm antibodies).
Cervix is a wonderful organ. It is lined by ducts which secrete the mucus. These ducts are again dependant on some hormones which determines the character of the mucus. During the time the egg is growing i.e. the follicular phase, the estradiol level is climbing but still not very high, the mucus is mostly thick scanty in nature.
Then as the egg approaches its maximum size and is about to rupture, the corresponding rise in estradiol leads to more watery and less viscous mucus which is easier for the sperms to negotiate. This is why you find thin watery mucus at time of ovulation. Then again after the egg ruptures progesterone is released. This converts the mucus back to a sticky form.
As explained earlier, cervix acts as the conscientious doorman allowing the sperms in during the ovulation phase in a slow trickle. While passing through the sperms are fed, made stronger and kind of rejuvenated for the journey ahead. Rest of the days, it is the impermeable defense not allowing anything and anyone to enter. However, this formula does go wrong in some where the cervical mucus actually kill off the sperms making it difficult for the couple to conceive. This is usually diagnosed by two methods. One is when we ask for the couple to have sex around the time of ovulation and then come to the clinic where we collect the mucus and check whether the sperms are moving or not. If all of them are dead, then possibly the mucus has the sperm killing substance. If they are alive then the mucus is not hostile. This is the post coital test.
The other way of knowing is when we check for the anti sperm antibodies in the semen or the blood of the man/woman. None of it is useful as it hardly correlates with the presence of the antisperm antibodies in the cervical mucus or inside the uterine cavity which is what we are actually looking for. But as yet that is not possible to test.
The simple solution for all suspected cases of hostile cervix is to put the semen beyond the cervix i.e. to perform an IUI. This alone takes care of all cervix related infertility. Some patients may still be having very high levels of such antibodies in the tubal fluid which would not allow fertilization but that is impossible to detect and is usually put under unexplained infertility. Attempts have been made to treat the condition with steroids hoping to bring down the levels of antibodies in the person but the results are dubious.
In short, all patients of mechanical factor infertility should rest assured that as because there is nothing wrong with the egg and the sperms pregnancy is certain. Though it might take an IUI to cross the cervix, or putting them together in IVF or rarely make the embryo grow in a surrogate’s uterus as because your uterus may be having lot of tumours. In all, pregnancy is bound to happen because egg and sperm are alright.
Perhaps this is last bastion of the reproductive endocrinologist. Whenever we cannot explain the infertility, we fall back on two tried and tested ruse- tuberculosis and unexplained. They are like chalk and cheese but they do bail us out of sticky situations especially if the patient is persistent.
Please understand there should not be any condition where we cannot tell you why pregnancy is not happening. But in reality, quite a few times we are stumped. Let us take the case of fibroids. As mentioned before, someone with lot of fibroids gets pregnant easily while someone with one tiny-winy fibroid fails to conceive at all. We can not but explain this as unexplained. What we mean actually is that these are not adequately researched or we do not know the reason as yet. Many a times we find good ovulation, decent semen but still no pregnancy. The standard tubal test has been found to be satisfactory. How to explain this? We say that maybe even if the tube is open, the eggs are not being picked up the tubes or there is improper sexual technique which is not reaching enough sperms into the vaginal canal. Sometimes the cervix may be hostile to the sperms. Now when we start treating this sort of a couple, we would ask for IUI for 3-4 months. If that brings about a pregnancy, then quite clearly, either the cervix or the sexual technique was at fault. If still no pregnancy, we ask for IVF. In an IVF cycle, enough eggs retrieved with satisfactory fertilization and great embryos are clearly suggestive of tubal problem as otherwise pregnancy should have occurred by now. So this way both baby making and finding out can go hand in hand
At other times very good patients not getting pregnant when put up for IVF show very poor fertilization. This has to do with the egg and sperm quality. This would have never been discovered if we hadn’t done IVF in these couples.
 Stories
Stories Knowledge centre
Knowledge centre Consulting
Consulting Team
Team