TUBE CHECKING
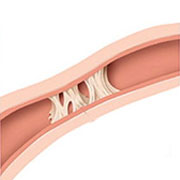
Tubal blockage is the least understood and most commonly made out reason for infertility. The fallopian tubes are mobile organs cylindrical in shape, attached to the uterus at one end and free at the other end. The free end has finger like projections which can catch the egg when it is released from the ovary. These eggs are then placed somewhere in the middle of the tube waiting for the sperms to reach. Now, if there are enough sperms which can make their way to the egg, then these sperms secrete two acids which dissolve the capsule around the egg allowing one sperm to go through into the egg to fertilize it. Thereafter, when the egg has become an embryo about 4-5 days old, there are hairs like projections (cilia) inside the lumen of the fallopian tube that push the embryo towards the other end into the uterine cavity for implantation. So, to reiterate, the tubes have three roles to play, pick up the egg, allow to sperms to come through and finally transfer the embryo to the uterine cavity. Two of these are dynamic activities which really cannot be assessed in any sure way. Only the fact that the sperms may not reach up to the egg can be commented upon by checking whether the tubes are open or not.
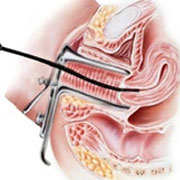
Tubes are open or not are again a little tricky to test. We do an hsg/ssg/laparoscopy to find out tubal status. But as mentioned before none of them is accurate. In quite a few cases, we are no wiser after the procedure. In all of the above procedures we rely on pushing water/dye into the uterus hoping that if tubes are open some of it would trickle out through their free end. So while tubes are not open for innocent sperms as they have no pressure to put, they open up miraculously in HSG/SSG when we do apply pressure to push the water/dye in. This is a dichotomy to be remembered always.
Also while we keep emphasizing tubal patency, we forget that tubo-ovarian relationship is just as crucial. If the tube and the ovaries are far apart, or as I have been stating again and again, somehow the tube and the ovaries are sticking to the back of the uterus and none is mobile then it is more at fault for the egg not finding its way into the tube rather than tubal block.
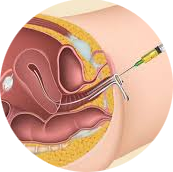
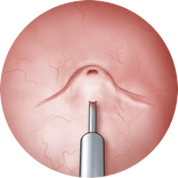
The straight and simple answer for all tubal factor infertility is IVF. But we could attempt other things provided duration of marriage is less than 5 years and the female is young. Tubal cannulation is a technique where a fine malleable catheter (pipe) is introduced into the fallopian tube from inside the uterine cavity. As it passes, it may take care of occasional blocks in the tube and create a sort of inner passage within the fallopian tube which if it maintains can allow sperms eventually to get to the egg. But as mentioned earlier, the success rate in terms of a pregnancy is not very encouraging because if the tubes are really damaged then opening them does not solve the problem as the hair like structures are not ok and would not transfer the baby back to the uterus when needed. We should attempt this in young women who have no known reason for picking up tubal damage such as past abdominal infection, appendicitis, chronic pelvic infections, history of TB etc.
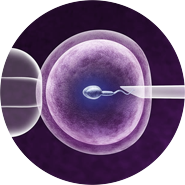
In all of rest, IVF currently offers the best possible chances at the least cost in terms of money and time.
Sometimes cases taken as unexplained infertility also eventually turn out to be tubal factor infertility. Because when we do IVF, we see that most of the eggs taken out have fertilized well and pregnancy happens quite easily with this technique whereas they had been toiling for last so many years with apparently everything ok.
 Stories
Stories Knowledge centre
Knowledge centre Consulting
Consulting Team
Team